
Category: Medicare
Taxpayers are funding California’s Medicaid shell game
Federal prosecutors in Minnesota have launched one of the largest Medicaid fraud crackdowns in American history. Raids. Indictments. Billions of dollars. A system designed to help the poor became a loot bag for criminals and grifters.
California saw those headlines and said, “They should have consulted us!”
Taxpayers don’t care whether fraud happens the Minnesota way — through day-care centers and nonprofits — or the California way — through health care accounting games.
Sacramento’s progressive class has spent years perfecting a cleaner version of the same scam — one that stays inside the lines, collects federal dollars on paper, and sends the bill to taxpayers everywhere else. Call it “legal.” Call it “approved.” Call it “routine.” None of those words makes it legitimate.
In 2004, the Government Accountability Office warned Congress that states were gaming Medicaid through intergovernmental transfers. States would shuffle public money through a circular process to make spending look real, inflate federal matching payments, then cycle the funds back to themselves. The GAO described “round-trip” arrangements that generated federal dollars without exposing states to true financial risk and that undermined the balance Congress intended.
Washington shrugged. Some states backed off. Others refined the trick.
California scaled it.
Medi-Cal, the state’s massive Medicaid program, now serves as the vehicle for this legal laundering operation. State officials insist that the system complies with federal rules. Fine. A loophole still remains a loophole, and taxpayers still pay the tab.
Paragon Health Institute, a conservative health policy organization, has laid out the mechanism clearly. Counties and public hospital systems transfer funds to the state through IGTs. The state counts that money as the “non-federal share” of Medicaid spending, then claims a larger federal match. Sacramento sends the combined state and federal funds back to government-owned providers through supplemental payments and formula-driven reimbursements.
The math almost always works in the contributors’ favor. The entities that send money in get reimbursed in full — and often receive more than they put up.
 Photo by Alex Wong/Getty Images
Photo by Alex Wong/Getty Images
California’s ambulance program shows how ugly this gets. Under the state’s Ground Emergency Medical Transport program, California bars payments from the state’s general fund. Public ambulance agencies instead receive “supplemental payments” that California largely restricts to public providers, limiting private companies’ access.
The result: California pays public ambulance providers about $1,065 per transport, while it offers private ambulance companies roughly $339 for the same job.
Then the federal government matches the inflated payments.
This isn’t just favoritism. It warps the market. It pushes private providers out and leaves patients with fewer options.
California has also expanded Medi-Cal eligibility regardless of immigration status. The state claims it funds routine coverage for “undocumented” adults with state dollars, but emergency Medicaid remains federally reimbursable. Sacramento still taps federal funds through the back door, even as it sells the program as a self-funded moral gesture.
This system stinks — even when regulators bless it.
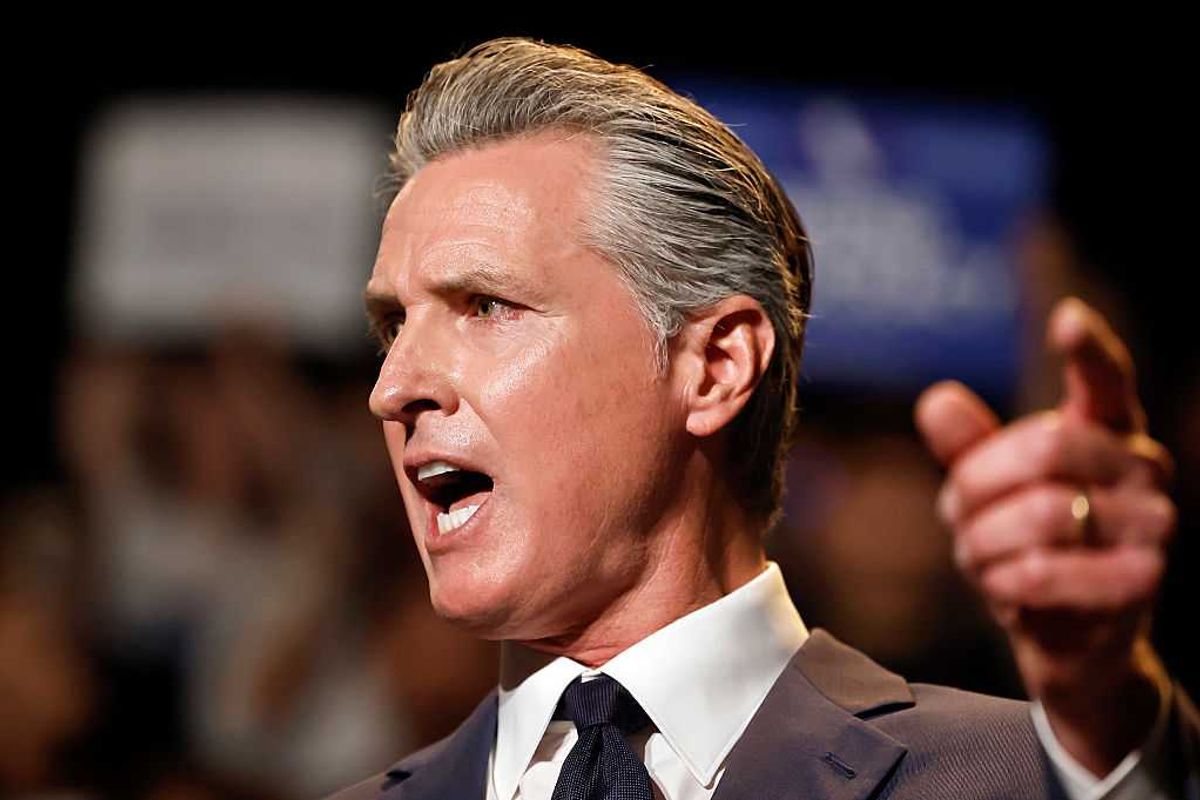
And the political contrast tells you everything. Minnesota’s fraud scandal has created enough public anger to drive its Democrat governor out of the next election. California Gov. Gavin Newsom (D), whose administration runs a program built on the same kind of federal exploitation — just with better paperwork — remains a top Democrat presidential prospect in 2028.
The federal government could stop this tomorrow. The Centers for Medicare and Medicaid Services could clamp down on the abuse of IGTs and demand a genuine state contribution, not an accounting illusion. Instead, under the Biden administration, CMS approved major expansions and encouraged the same incentives that fuel the problem.
Audits don’t fix it, either. Regulators review what states claim on paper, not what taxpayers actually fund. If a state can justify the scheme in bureaucratic language, CMS signs off. Fraud analysis often misses the point for the same reason. A state can structure IGTs so the “state share” exists largely as a bookkeeping device. Federal taxpayers remain the only party exposed to real financial loss.
Congress never designed Medicaid to serve as a revenue stream for local governments. It created Medicaid to help the poor. California’s 12-to-1 payment disparities punish the poor by reducing competition, shrinking access, and driving private providers out of business.
RELATED: The insane little story that failed to warn America about the depth of Somali fraud
 Tom Williams/CQ-Roll Call Inc. via Getty Images
Tom Williams/CQ-Roll Call Inc. via Getty Images
Congress already has the solution. The GAO outlined it two decades ago, and the George W. Bush administration backed the basic idea: Close the loophole by prohibiting Medicaid payments that exceed actual costs for government-owned facilities.
In plain English: Stop rewarding government-owned providers with inflated reimbursements that private providers can’t touch. Set equal rules. Require real state contributions. Cut the circular funding schemes that turn Medicaid into a federal ATM.
Taxpayers don’t care whether fraud happens the Minnesota way — through day cares and nonprofits — or the California way — through health care accounting games. We care that Washington keeps subsidizing systems designed to break the rules everyone else has to follow.
California built this machine. Congress can shut it down.
Medicaid’s 30-Year Refusal to Stop Funding the Dead
For more than 30 years, Washington has known that Medicaid hemorrhages taxpayer dollars through fraud, waste, and abuse, including payments…
For once, Medicare is trying something that actually saves money

Medicare is the second-largest program in the federal budget, topping $1 trillion last year. In 2023, it accounted for 14% of federal spending — a share projected to reach 18% by 2032. After years of ballooning costs, something is finally being done to slow the growth. A new Medicare pilot program, the Wasteful and Inappropriate Service Reduction model, borrows a successful private-sector tool: prior authorization. And that’s good news.
Medicare Part B premiums now sit at $185 per month — up 28% from five years ago and a staggering 76% since 2015. Last year, 12% of the 61 million Americans enrolled in Part B spent more than a tenth of their annual income on premiums. That burden is unsustainable.
In a system as expensive and fragmented as ours, no one can afford to keep writing blank checks for low-value care.
WISeR, set to launch in Ohio, Texas, Washington, New Jersey, Arizona, and Oklahoma, will require prior approval for a short list of “low-value” services — procedures that research shows are frequently overused, costly, and sometimes harmful.
To some, the idea of Medicare reviewing certain treatments before covering them may sound like red tape. But when done correctly, prior authorization is not a barrier. It is a guardrail — one that protects patients, improves quality, and helps ensure that both tax dollars and premiums are spent appropriately.
The goal of WISeR is simple: Cut unnecessary treatments and shift resources toward more effective, evidence-based care. Critics warn about the possibility of delays or extra paperwork, and those concerns are worth monitoring. But they don’t negate prior authorization’s potential to make U.S. health care safer, more efficient, and more financially stable.
Prior authorization directly targets some of the most persistent problems in health care. Medicare spends billions each year on low-value services. A 2023 study identified just 47 such services that together cost Medicare more than $4 billion annually. Those are taxpayer dollars that could be put to better use.
The private insurance market shows the same pattern: unnecessary imaging, avoidable specialist referrals, and brand-name drugs chosen over generics all contribute to rising premiums. Prior authorization, when used properly, reins in this waste by ensuring coverage lines up with medical necessity and evidence-based best practices. Research from the University of Chicago shows that Medicare’s prior authorization rules for prescription drugs generate net savings even after administrative costs.
Consider one striking example. Medicare Part B covers wound-care products known as skin substitutes. But an Office of Inspector General report found that expenditures on these products skyrocketed over the past two years to more than $10 billion annually. Meanwhile, Medicare Advantage plans — which rely heavily on prior authorization — spent only a fraction of that amount for the same treatments.
RELATED: When a ‘too big to fail’ America meets a government too broke to bail it out
 DNY59 via iStock/Getty Images
DNY59 via iStock/Getty Images
More importantly, prior authorization helps promote evidence-based medicine. It curbs outdated clinical habits and reduces financial incentives to overtreat. Health plans consistently say that prior authorization aligns care with gold-standard clinical guidelines, particularly in areas prone to misuse.
Of course, the system must be designed responsibly. A well-functioning PA process should be transparent, fast, and grounded in strong clinical evidence. Decisions should be made in close coordination with the patient’s treating provider. The appeals process must be straightforward. And both public and private payers should be held accountable for improper denials or harmful delays.
When structured this way, prior authorization is far more efficient than the current “pay-and-chase” model, where Medicare pays first and tries to recover improper payments later.
Prior authorization already works in the private sector. It can work in Medicare.
Public and private payers have an obligation to steward the dollars they spend — whether those dollars come from taxpayers or premium-payers. In a system as expensive and fragmented as ours, no one can afford to keep writing blank checks for low-value care. When implemented wisely, prior authorization keeps coverage aligned with medical necessity, elevates the value of care, and helps deliver better outcomes at a sustainable cost.
Do We Really Need to Slash the Debt?
John Tamny, the free-market economics commentator who edits RealClearMarkets, comes out swinging in The Deficit Delusion: Why Everything Left, Right, and Supply-Side Tells You About the National Debt Is Wrong. Perhaps this isn’t surprising, given the book’s title. It can feel like Tamny is a kid walking through the elementary-school playground, randomly shoving other kids—some of whom are bigger than he—as he attacks one op-ed writer after another for, allegedly, misunderstanding the national debt.
The post Do We Really Need to Slash the Debt? appeared first on .
Fearmongering over Medicare hides the real fix seniors need

Democrats are casting the shutdown showdown as a battle over health care costs, tapping into widespread anxiety over the cost of health care, especially among those enrolled in Medicare. For them, it’s politics. But for millions of American seniors, the worry is real — not just a convenient talking point.
Recent polling shows 58% of Medicare recipients 65 and over are concerned about future health care costs, and half are worried a major health situation could result in either debt or bankruptcy.
If left unchanged, Medicare will be unable to pay full benefits by 2036.
While medical debt is a growing concern among Medicare recipients, the staggering size of the federal debt — largely driven by Medicare spending — is a ticking time bomb Congress can no longer ignore. As one of the largest federal spending programs, Medicare consisted of a jarring $874 billion out of the $6.75 trillion federal budget (about 13 cents of every dollar spent in FY2024).
While Medicare receives some funding from premiums paid by enrollees, the single largest source of revenue comes from the federal government’s general fund. If left unchanged, Medicare will be unable to pay full benefits by 2036.
Medicare Advantage toes the line
Fortunately, policy solutions exist that can help both seniors and taxpayers.
Medicare Advantage merges public financing with private delivery under accountability. The government pays a fixed amount per enrollee to private plans, calibrated by benchmarks and quality measures. Plans that achieve higher star ratings — which were just released for 2026 by the Centers for Medicare and Medicaid Services earlier this month — receive bonus payments. Meanwhile, poor performers lose ground.
This structure introduces incentives for efficiency and quality that are lacking in traditional Medicare. Yet, successive years of cuts to how Medicare Advantage plans are reimbursed have forced several major insurers to announce they’re withdrawing from certain Medicare Advantage markets next year.
Companies like UnitedHealth, Humana, Aetna, as well as regional plans such as UCare (serving Minnesota and parts of Wisconsin) and Blue Cross Blue Shield of Vermont, are withdrawing from select Medicare Advantage counties across the country, citing rising costs. Seniors are using more medical services than expected, driving up claims, while federal reimbursement rates are being cut. Added regulatory and administrative burdens (such as expanded reporting requirements and prior authorization rules) further limit insurers. Together, these pressures make participation unsustainable in some markets.
If unchanged, more insurers will leave Medicare Advantage, and options for seniors will continue to shrink. Meanwhile, Medicare costs are growing much faster than private health care spending.
In 2023, traditional Medicare spent $15,689 per enrollee, more than double the private sector amount. This is a result of the traditional fee-for-service model, which pays providers per treatment instead of per patient, rewarding volume over outcomes, encouraging unnecessary care, and driving up costs.
Conversely, Medicare Advantage’s structure encourages prevention and coordination. To attract enrollees, Medicare Advantage offers supplemental benefits such as vision, dental, hearing, wellness programs, transportation, and over‑the‑counter benefits. Many Medicare Advantage plans now include these extras at little or no additional cost. That flexibility helps tailor benefits to beneficiary needs.
Better treatment, lower costs
When allowed to work, Medicare Advantage delivers higher satisfaction, lower costs, and greater access to coverage than traditional Medicare. One Harvard study found that seniors enrolled in Medicare Advantage had better health outcomes than seniors on traditional Medicare. A National Institutes of Health review of hundreds of studies found that Medicare Advantage provided significantly better quality of care and health outcomes than traditional Medicare by a factor of four to one. Another NIH study found that across 48 studies, Medicare Advantage enrollees received more preventative care and had fewer hospitalizations and emergency visits, shorter stays, and lower total spending.
The financial and quality advantages are clear. One study comparing expected out‑of‑pocket costs in Medicare Advantage versus traditional Medicare found that from 2014 to 2019, projected costs were 18% to 24% lower under Medicare Advantage. For seniors on fixed incomes — that is significant.
RELATED: Democrats deny shutdown is about health care for illegal aliens — then one admits the truth
 Photo by Nathan Posner/Anadolu via Getty Images
Photo by Nathan Posner/Anadolu via Getty Images
Seniors get it. This year, the majority of Medicare beneficiaries are enrolled in Medicare Advantage plans. Over the last two decades, enrollment in Medicare Advantage has skyrocketed. Unsurprisingly, polling shows 93% of Medicare Advantage enrollees were satisfied or very satisfied with their coverage, and 94% would recommend it to their family and friends. The Congressional Budget Office now projects that by 2034, Medicare Advantage could account for nearly two-thirds of all Medicare beneficiaries.
The model for the future
Medicare Advantage provides the model for quality, affordable health care for seniors that aligns with what they prefer. Reducing regulatory burdens and barriers within the insurance market will provide Medicare Advantage plans greater flexibility and even entice those insurers leaving the Medicare Advantage market to reconsider.
Medicare cannot continue as purely fee‑for‑service without reform — neither for the medical and financial health of Americans, nor for the sake of the federal budget. The current fiscal challenges plaguing the federal budget demand models that can bend the cost curve while improving quality. Medicare Advantage is not a cure-all, but it is among the most promising tools in the toolbox.


